I have reproduced it in its entirety here so that I could add emphasis... Sooo italics and boldface are mine except as noted.
___________________________________________________________________
Manipulation under Anesthesia: Neurological Effects of Different Modes of Anesthesia
By Brad McKechnie, DC, DACAN
The purpose of this article is to lend some insight into the neurological effects of general anesthetic regimens and sedative/hypnotic regimens employed during manipulation under anesthesia.
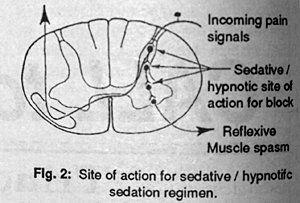
Thus, two key areas for paraspinal muscle spasm production and pain transmission within the spinal cord are affected: internuncial neuronal reactions; and myoneural junction. By depressing internuncial neuronal transmission within the spinal cord, the pathology producing the abnormal muscle spasm is taken out of contact with the alpha motoneurons located in the anterior horn of the spinal cord's gray matter. The alpha motoneurons are responsible for producing activity in skeletal muscle.

In the intact pain-spasm-pain cycle, the site of the spinal or paraspinal pathology is reflexively linked to the alpha motoneurons in the cord's anterior horn, leading to a reflexive muscle spasm in response to pain (Figure 1). By temporarily depressing this activity within the spinal cord via administration of sedative/hypnotic medications, one key pathway for the facilitation of paraspinal muscle spasm is removed. As these substances also affect the myoneural junction by depressing skeletal muscle transmission, the flaccid paralysis of the paraspinal muscles necessary for the MUA procedure is enhanced (Figure 2). (Please note that the desired reaction (flaccid paralysis) is merely ENHANCED by Versed. This can be done without the permanent mental disruption of Versed...)
Sodium Pentothal produces induction of anesthesia within 60 seconds of administration, reflecting its rapidity of central nervous system penetration. The patient's blood pressure will decrease during the procedure and the heart rate will increase. Awakening from sodium Pentothal reflects the redistribution of the drug from the central nervous system to inactive tissue sites in fat and skeletal muscle. Sodium Pentothal's liver clearance rate is from 15-20 percent per hour. Should this procedure of sedation be utilized for a patient treated on an outpatient basis, it is necessary for someone to accompany the patient to the outpatient facility that will be able to drive the patient home after the procedure.
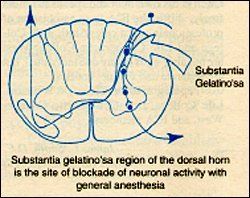
Patients sedated with sodium Pentothal may report amnesia for events occurring during the procedure. Versed has effects similar to those of sodium Pentothal with the exception that the memory loss for events occurring during the procedure is greater than with sodium Pentothal. In contrast, general anesthetics produce graded depression of all levels of central nervous system function by increasing the threshold at which firing occurs, thereby decreasing transmission. General anesthetics create a blockade of neuronal activity within the substantia gelatino'sa of the spinal cord's dorsal horn. The substantia gelatino'sa is the site which receives incoming nociceptive impulses entering the spinal cord. From this location, the noxious pain impulses are sent to the cortex via the lateral spinothalmic tact and to the anterior horn at the corresponding segmental level to create muscle spasm to the muscle or muscles acting over the joint or area serving as the origin of the pain impulse (Figure 3).
The alteration of central nervous system function by general anesthesia follows a pattern characterized as a combination of ascending and descending depression of the central nervous system that spares the medullary centers unless large doses of anesthetics are used (Figure 4).
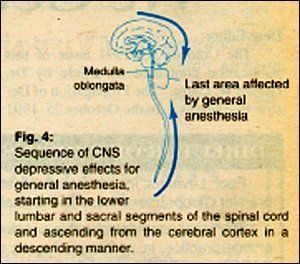
The first areas of the central nervous system affected by general anesthetics are the lower segments of the spinal cord and the cerebral cortex. With more intense levels of the anesthetics, the central nervous system depressive effects spread upward through the spinal cord and downward through the subcortical and mid-brain levels to converge on the medullary centers which house the autonomic centers necessary for vegetative function, and on the cervical spinal cord region supplying motor function to the diaphragm via the phrenic nerve.
Due to the more complex technical nature and risk factors of general anesthesia, it does not share the popularity of the sedative/hypnotic method of anesthesia for the MUA procedure.
References
- Myers FH, Jawtez E, and Goldfein A: Review of Medical Pharmacology, ed 7. Lange Medical Publishers, Los Altos, California, 1980.
- Katsung BG: Basic and Clinical Pharmacology. Lange Medical Publishers, Los Altos, California, 1982.
- Stoelting RK, Miller RD: Basics of Anesthesia. Churchill-Livingstone, New York, 1984.
Brad McKechnie, D.C., D.A.C.A.N.
Pasadena, Texas
___________________________________________________________________
No comments:
Post a Comment